Dental fillings – How invisible!
Invisible fillings
Caries can develop despite good dental care. At the latest when this has reached the dentin, the dentist must remove the caries with a drill and close the hole, the so-called cavity, with a filling. Thanks to modern materials and developments in dentistry and dental technology, there is now a wide range of different materials and techniques available. The type of dental filling and the material used depend primarily on the extent of the damage and the location of the affected tooth, but also on the patient’s wishes and requirements. Filling therapy is one of the most common dental treatments. In addition to repairing the defect, the aesthetic restoration of the tooth is the primary goal of filling therapy.
At Leipziger-Ihre Zahnärzte we only use tooth-coloured and biocompatible filling materials.

1. plastic (direct) fillings
1.1. Composite (ceramic-reinforced plastic) – natural and gentle
Composites are tooth-coloured and can be easily matched to the natural enamel shade. Fillings can be designed with nature-identical colour gradations and transparencies. An inconspicuous tooth repair is therefore possible. They are pressure and fracture resistant so that they can also be used on the occlusal surfaces. The application is technically demanding and time-consuming. Due to their good aesthetics, they are also suitable for restoring incisors, canines and posterior teeth.
A simple composite filling is usually sufficient for minor caries damage. For larger or deeper holes, the dentist is more likely to apply a layered composite filling. This is also possible in a single treatment session. To perfectly reproduce the natural tooth colour, the composite layers can have different colour intensities (multi-colour technique).
Requirements for a contemporary, durable composite for the posterior region
- Highest possible proportion of ceramic particles to achieve good mechanical properties
- “Radiopacity”, i.e. recognisability of the filling in the X-ray image in order to be able to make statements regarding possible caries development at the edge or under the filling
- Good polishability to minimise plaque build-up on the composite filling
- Extremely low shrinkage behaviour even under the influence of spokes
Resulting advantages of composite at a glance
- “Invisible”, thanks to natural colour matching
- Can be used in the anterior and posterior region
- Combination of very good stability and gloss retention
- Very good sealing
- High abrasion resistance and durability
- loadable in the chewing area
- Good biocompatibility
- Gentle caries therapy
How are composite fillings placed in the tooth?
1. simple composite filling

2. layered composite filling (multi-layer technique) or combination of multi-layer technique and multi-colour technique for the highest demands
The enamel area at the cavity is bevelled to increase the bonding surface. After the tooth has been drained, the enamel and dentin are cleaned with a phosphoric acid and an adhesive layer is applied. Anschließend wird die weiche Füllmasse in Schichten von etwa 2 mm (Mehrschichttechnik) in die Kavität eingebracht, wobei mit verschiedenen Farbnuancen (Mehrfarbtechnik) gearbeitet und jede Schicht einzeln mit Blaulicht ausgehärtet wird. By processing the composites in layers, we model an “invisible” filling true to nature and achieve optimum naturalness.

The dentist uses articulating paper (blue paper) to adapt the finished filling to the bite block. After you have bitten on it with different tooth and jaw positions, the dentist can see the points of contact and can thus determine whether and where the filling still needs to be corrected.
Durability of composite fillings
Limits of composite fillings
2. hard (laboratory-made) inlay fillings
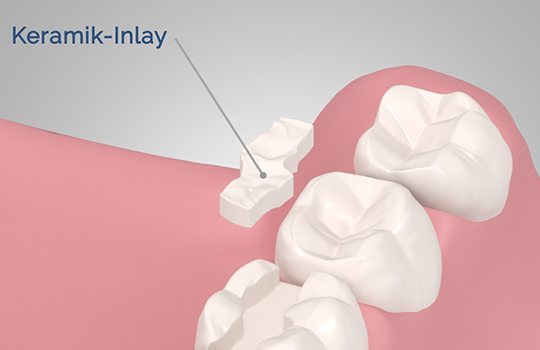
2.1. Ceramic inlay – invisible, durable and high strength
Until the inlay is ready, the tooth is initially treated with a temporary filling.
Overall, the preparation and placement of the filling is quite demanding, time-consuming and cost-intensive. From an aesthetic point of view, however, ceramic inlays fulfil the highest demands. Whether glass-ceramic, oxide or zirconium oxide ceramic – all are dimensionally stable, abrasion-resistant, tooth-coloured, translucent and therefore invisible as fillings. The inlay can be customised precisely to the tooth and also impresses in terms of durability and compatibility. It enables a good edge seal because there is no shrinkage due to the curing process.
Advantages of ceramic at a glance
- Very good function (abrasion like natural tooth enamel)
- Stabilising effect through adhesion to the tooth structure
- Very good aesthetics
Disadvantages of ceramics at a glance
- Integration more complex than with gold
- Brittle, low flexural strength, not absolutely break-proof
2.2. Gold inlay – shatterproof, but not invisible
However, the dental filling material with the longest tradition is and remains gold. Gold is very well tolerated by the body and has a long service life. Since pure gold cannot withstand the chewing pressure, alloys with platinum, palladium, silver or copper are used for dental fillings.
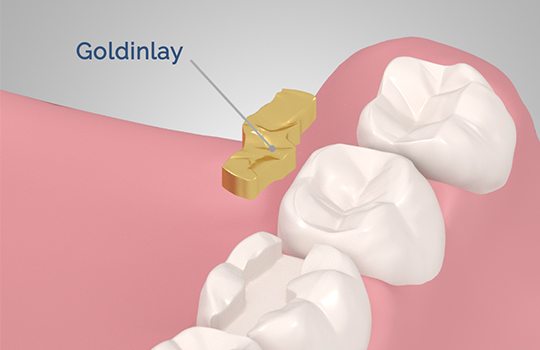
The disadvantage of gold fillings is their conspicuous appearance, which is why aesthetic ceramic inlays are increasingly being used in the anterior region. In addition, the teeth have to be ground down comparatively heavily, so gold inlays are rather unattractive for the repair of small defects.
Advantages of gold at a glance
- Very good function
- Absolutely unbreakable
- is not adhesively bonded to the tooth and can therefore weaken the remaining tooth substance
Disadvantages of gold at a glance
- Very conspicuous, therefore loss of aesthetics
- more substance removal than with ceramic restorations
3. other types of filling material
Glass ionomer cement (cement filling) (GIZ) – “temporary solution”
Compomer filling – for smaller defects
Plastic inlay
Selecting the right filling

Patient OPINIONS
Great doctor
Thorough diagnosis; honest recommendation not to carry out the planned special treatment in my case, thus saving me unnecessary treatment costs.
Friendly and competent
I felt safe and in good hands from the very first moment. Dr Planert took the time to answer my questions and explained everything clearly.
Outstanding!
I am completely satisfied! Very courteous reception... Advice and treatment at a very high level. Can recommend Leipziger14-Ihre Zahnärzte and Mr Planert with a clear conscience!"
Great doctor
Thorough diagnosis; honest recommendation not to carry out the planned special treatment in my case, thus saving me unnecessary treatment costs.
Outstanding!
I am completely satisfied! Very courteous reception... Advice and treatment at a very high level. Can recommend Leipziger14-Ihre Zahnärzte and Mr Planert with a clear conscience!"
Friendly and competent
I felt safe and in good hands from the very first moment. Dr Planert took the time to answer my questions and explained everything clearly.




